Developing competent patient assessment skills is critical to delivering appropriate patient care. Remember to always look at your patients, talk to them, explore the clinical picture before anything else.
Almost every part of assessment relates to one of these four critical life functions:
Oxygenation (increase FiO2)
Circulation (chest compression, defribrillate, heart drugs, ect.)
Perfusion (increase BP).
*The most common problem is with oxygenation.
Here are some helpful visuals for assessment I thought I would share...
Almost every part of assessment relates to one of these four critical life functions:
- Ventilation: breathing air in and out of lungs. Vital signs-> respiratory rate (RR), tidal volume, chest movement, breath sounds, PaCO2
- Oxygenation: getting O2 into the blood. Vital signs-> heart rate (HR), color, sensorium, PaO2
- Circulation: moving the blood through the body. Vital signs-> pulse/HR and strength, cardiac output (C.O.)
- Perfusion: getting blood and O2 into the tissue. Vital signs-> blood pressure (BP), sensorium, temperature, urine output, hemodynamics
Oxygenation (increase FiO2)
Circulation (chest compression, defribrillate, heart drugs, ect.)
Perfusion (increase BP).
*The most common problem is with oxygenation.
Here are some helpful visuals for assessment I thought I would share...
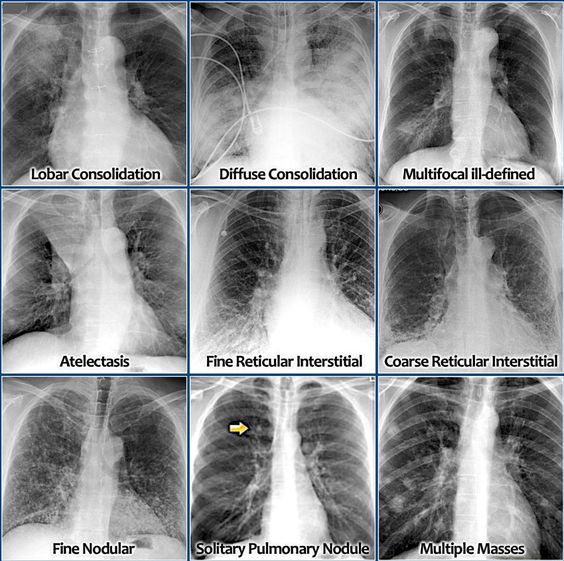
- Infiltrate--> Atelectasis
- Consolidation--> Pneumonia, Pleural Effusions
- Hyperlucency--> COPD, Asthma attack, PTX
- Vascular Markings--> increased with CHF, absent with PTX
- Fluffy infiltrates, Butterfly/Batwing pattern--> Pulmonary Edema
- Ground Glass appearance/Honeycomb pattern--> ARDS/ILD
- Air Bronchgram--> Pneumonia
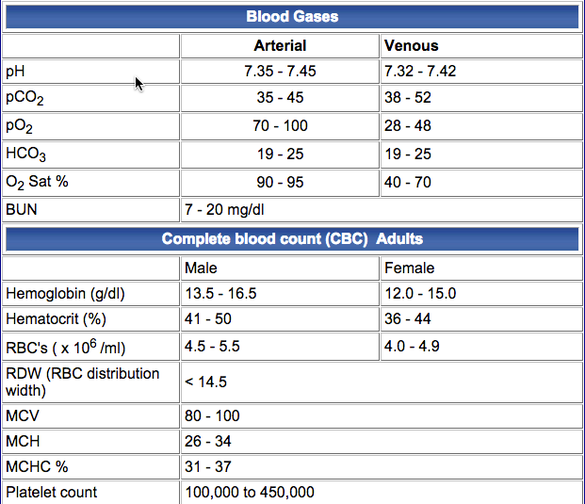
Blood tests are performed to evaluate the general health status of a patient, identify organ system dysfunction, detect the presence of infection, and determine the effects of therapy. Being able to recognize how some abnormalities influence pulmonary function is crucial in assessing your patient as an RT.
Some common correlations:
Some common correlations:
- Hypokalemia (low potassium)-->metabolic alkalosis, excessive excretion, renal loss, vomiting, flattened T waves on EKG.
- Hyperkalemia (high potassium)--> kidney failure, spike T wave (metabolic acidosis)
- Hyponatremia (low sodium)--> fluid loss from: diuretics, vomiting, diarrhea. Fluid gain from: CHF, IV therapy
- Hypernatremia (high sodium)--> dehydration
- Hypochloremia (low chloride)--> metabolic alkalosis
- Hyperchloremia (high chloride)--> metabolic acidosis
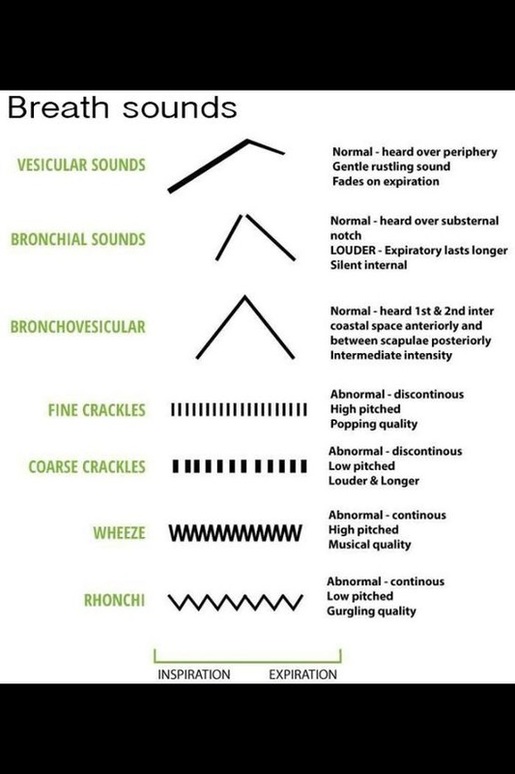
Auscultating a patient is a vital part of patient assessment and can indicate the underlying problem. For example abnormal breath sounds such as crackles is indicative of secretions/fluid. Fine crackles is fluid in alveoli, the patient may have CHF or pulmonary edema and treatment may include IPPB, heart drugs, diuretics and oxygen. Coarse crackles indicates large airway secretions and the patient needs suctioning. Wheezes are due to bronchospasm and the patient needs a bronchodilator. Unilateral wheeze is indicative of a foreign body obstruction.
Two abnormal breath sounds not mentioned in the above image are stridor (harsh, high-pitched noise on inspiration) which is due to upper airway obstruction. Stridor is often heard with subglottic swelling conditions such as Croup (a viral disorder common in infants and young children) and post extubation. Stridor can also be heard in Epiglottis (a potentially life-threatening inflammation of the supraglottic airway caused by a bacterial infection. Treatment for stridor is typically racemic epinephrine (for swelling and edema). In addition, pleural friction rub (a coarse grating or crunching sound) is another type of breath sound caused by inflamed surface of the visceral and parietal pleura rubbing together. Drugs such as steroids and antibiotics are indicated.
Two abnormal breath sounds not mentioned in the above image are stridor (harsh, high-pitched noise on inspiration) which is due to upper airway obstruction. Stridor is often heard with subglottic swelling conditions such as Croup (a viral disorder common in infants and young children) and post extubation. Stridor can also be heard in Epiglottis (a potentially life-threatening inflammation of the supraglottic airway caused by a bacterial infection. Treatment for stridor is typically racemic epinephrine (for swelling and edema). In addition, pleural friction rub (a coarse grating or crunching sound) is another type of breath sound caused by inflamed surface of the visceral and parietal pleura rubbing together. Drugs such as steroids and antibiotics are indicated.
Hopefully this was helpful! I am learning everyday in clinicals that you can't rely on the monitors or just looking at patient's charts- you learn more about a patient's condition by simply using your observation skills and picking up on abnormal findings. Also- if you can, just talk to your patients, often times they will open up to you more than their physician. You not only learn more about their specific condition but learn the best plan of action for your patient. It is always about the patient!!


 RSS Feed
RSS Feed
