
In light of April being National Sarcoidosis Awareness Month I wanted to do a post talking about Sarcoidosis. So what is Sarcoidosis? Sarcoidosis is a multisystemic autoimmune inflammatory disease in which lymphocytes become overactive. These overactive lymphocytes release chemical substances which cause noncaseating granulomas in various organs in the body. This disease is of particular interest to a respiratory therapist because in 90% of cases the lungs are affected. Other common organs involved include the lymph glands, skin, and eyes.
The clinical picture of sarcoidosis can be complicated by intermittent inflammation in many different organs, making diagnosis difficult. Several cases are actually incidentally diagnosed by a chest x-ray because approximately 30-50% of patients are asymptomatic.
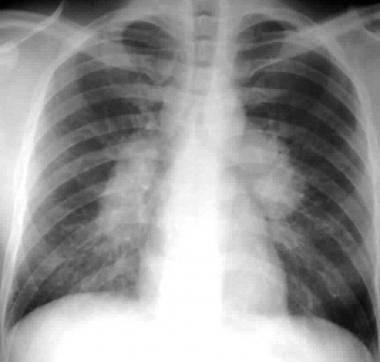
CXR findings categorizes the 5 stages of Sarcoidosis:
Stage 0= Normal CXR (although normal, this does not exclude diagnosis, particularly when cardiac or neurologic involvement is suspected)
Stage 1= bilateral hilar lymphadenopathy
Stage 2= bilateral hilar lymphadenopathy and infiltrates
Stage 3= infiltrates alone
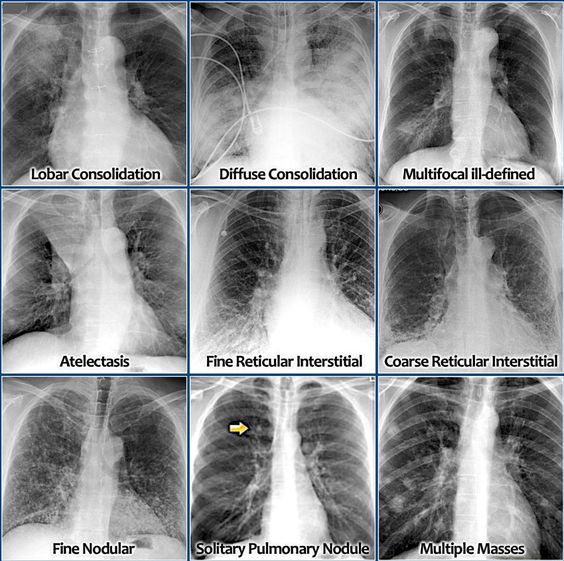
Stage 4= fibrosis [honey-combing- reticulonodular pattern]
Exclusion of other diseases that may produce a similar histological or clinical picture such as TB, lupus, and histoplasmosis is critical. To exclude hypersensitivity pneumonitis the CD4+/CD8+ ratio is assessed through bronchoalveolar lavage (BAL) fluid analysis. An inverted ratio > 4:1 will suggest pulmonary Sarcoidosis and a ratio <1 will suggest hypersensitivity pneumonitis. The most accurate diagnostic test is a biopsy which will show evidence of noncaseating granulomas and also definitively differentiate sarcoidosis from lymphoma. Sarcoidosis is often referred to as the ‘snowflake’ disease because patients present with so many different symptoms. Symptoms vary from patient to patient depending on which organ system is involved. General symptoms include: fatigue/weakness, night sweats, low-grade fever, weight loss, joint pain, and sleeping difficulties. Most common symptoms associated with pulmonary involvement are dry or productive cough, dyspnea, chest pain or pressure, and SOB. If you think about it these symptoms make sense considering the granulomas in the lung are taking over the alveoli affecting gas exchange.
Assessment of the degree of pulmonary involvement includes PFTs, CXR or CT scan, and subjective or measured scale of dyspnea. Pulmonary Function Tests results are often normal in early stages but in advanced stages a restrictive pattern with decreased vital capacity, TLC, and DCLO is typically present. However, in 15-20% an obstruction may be present due to enlarged chest lymph nodes compressing the airway, and/or the granulomas themselves. The six minute walk test (6MWT) is useful for both predicting mortality and monitoring response to therapy. Distance is reduced in the majority of patients and correlates with reductions in FVC and ambulatory pulse ox saturation. A DCLO of less than 60% predicted plus oxygen desaturation of less than 90% on the 6MWT equals a high likelihood of pulmonary hypertension. In addition, High resolution CT scan is more sensitive for the detection of enlarged lymph nodes. Identifies alveolitis verses fibrosis.
Treatment for sarcoidosis is designed to slow down the development of granulomas and to relieve the various ailments depending on the symptoms. Indications for treatment include: progressive pulmonary or extrapulmonary involvement, cardiac, CNS, eye involvement, and persistent hypercalcemia. Corticosteroids are the first line of treatment, usually Prednisone in high doses. Prednisone suppresses the immune system so the granulomas can shrink in size and allow normal tissue of the organs to take over. Due to the numerous side effects of Prednisone, the dose should be tapered over a 6-month course and eventually discontinued. Steroid-sparing agents such as Methotraxate can be used as an alternative when Prednisone is ineffective or cause unacceptable side effects. Furthermore, to treat cutaneous lesions, hypercalcemia, neurologic sarcoidosis and bone lesions antimalarial drugs such as Chloroquine are prescribed. Medications such as Albuterol, Flovent, and Pulmicort are used to relieve pulmonary symptoms. Lung and cardiac transplantation is reserved for end-stage disease. Effective treatment involves collaboration between all the patient's physicians.
The clinical picture of sarcoidosis can be complicated by intermittent inflammation in many different organs, making diagnosis difficult. Several cases are actually incidentally diagnosed by a chest x-ray because approximately 30-50% of patients are asymptomatic.
CXR findings categorizes the 5 stages of Sarcoidosis:
Stage 0= Normal CXR (although normal, this does not exclude diagnosis, particularly when cardiac or neurologic involvement is suspected)
Stage 1= bilateral hilar lymphadenopathy
Stage 2= bilateral hilar lymphadenopathy and infiltrates
Stage 3= infiltrates alone
Stage 4= fibrosis [honey-combing- reticulonodular pattern]
Exclusion of other diseases that may produce a similar histological or clinical picture such as TB, lupus, and histoplasmosis is critical. To exclude hypersensitivity pneumonitis the CD4+/CD8+ ratio is assessed through bronchoalveolar lavage (BAL) fluid analysis. An inverted ratio > 4:1 will suggest pulmonary Sarcoidosis and a ratio <1 will suggest hypersensitivity pneumonitis. The most accurate diagnostic test is a biopsy which will show evidence of noncaseating granulomas and also definitively differentiate sarcoidosis from lymphoma. Sarcoidosis is often referred to as the ‘snowflake’ disease because patients present with so many different symptoms. Symptoms vary from patient to patient depending on which organ system is involved. General symptoms include: fatigue/weakness, night sweats, low-grade fever, weight loss, joint pain, and sleeping difficulties. Most common symptoms associated with pulmonary involvement are dry or productive cough, dyspnea, chest pain or pressure, and SOB. If you think about it these symptoms make sense considering the granulomas in the lung are taking over the alveoli affecting gas exchange.
Assessment of the degree of pulmonary involvement includes PFTs, CXR or CT scan, and subjective or measured scale of dyspnea. Pulmonary Function Tests results are often normal in early stages but in advanced stages a restrictive pattern with decreased vital capacity, TLC, and DCLO is typically present. However, in 15-20% an obstruction may be present due to enlarged chest lymph nodes compressing the airway, and/or the granulomas themselves. The six minute walk test (6MWT) is useful for both predicting mortality and monitoring response to therapy. Distance is reduced in the majority of patients and correlates with reductions in FVC and ambulatory pulse ox saturation. A DCLO of less than 60% predicted plus oxygen desaturation of less than 90% on the 6MWT equals a high likelihood of pulmonary hypertension. In addition, High resolution CT scan is more sensitive for the detection of enlarged lymph nodes. Identifies alveolitis verses fibrosis.
Treatment for sarcoidosis is designed to slow down the development of granulomas and to relieve the various ailments depending on the symptoms. Indications for treatment include: progressive pulmonary or extrapulmonary involvement, cardiac, CNS, eye involvement, and persistent hypercalcemia. Corticosteroids are the first line of treatment, usually Prednisone in high doses. Prednisone suppresses the immune system so the granulomas can shrink in size and allow normal tissue of the organs to take over. Due to the numerous side effects of Prednisone, the dose should be tapered over a 6-month course and eventually discontinued. Steroid-sparing agents such as Methotraxate can be used as an alternative when Prednisone is ineffective or cause unacceptable side effects. Furthermore, to treat cutaneous lesions, hypercalcemia, neurologic sarcoidosis and bone lesions antimalarial drugs such as Chloroquine are prescribed. Medications such as Albuterol, Flovent, and Pulmicort are used to relieve pulmonary symptoms. Lung and cardiac transplantation is reserved for end-stage disease. Effective treatment involves collaboration between all the patient's physicians.
FUN FACTS!
- Sarcoidosis is derived from the Greek root meaning “flesh-like”; cutaneous lesions of the disease often fit this description
- The disease was discovered more than 100 years ago by two dermatologists




















 RSS Feed
RSS Feed
